Pattern hair loss is the most prevalent type of progressive thinning globally, impacting men and women of all ethnicities. However, the pattern and timeline vary from person to person. This progressive form of thinning is what clinicians describe as pattern hair loss.
This form of hair loss, unlike sudden diffuse shedding that usually improves with trigger correction, is gradual and influenced by heredity and hormones. This covers what to know about the condition, its presentation in men and women, and typical management.
What Is Androgenetic Alopecia and How It Develops
Androgenetic alopecia is a hereditary, hormone-mediated condition that causes progressive miniaturization of hair follicles. Thick terminal hairs become finer, shorter, and weaker across successive hair cycles. Over time, some follicles may produce only very fine hair or become clinically inactive. But it is distinctive in that the pattern is typically gradual and localized to specific zones of the scalp, rather than the diffuse whole-scalp shedding seen in telogen effluvium.
The central biological driver here is dihydrotestosterone (DHT). It is not always about elevated hormone levels; patients often have normal hormone levels but carry genetic variants that make their follicles more sensitive to androgen signaling. Because of this, early recognition is key because miniaturized follicles can still be biologically active and may respond to treatment.
What Causes Androgenetic Alopecia
Genetic Predisposition
Androgenetic alopecia is polygenic. This means that multiple genes contribute to the condition rather than a single “hair loss gene.” Family history from either side of the family may be relevant, though relatives can differ in pattern and severity.
Androgen Sensitivity at the Follicle
DHT binds to androgen-sensitive follicles and progressively shortens the growth phase of the hair cycle. Successive cycles produce thinner and shorter hairs, a process known as follicular miniaturization.
Hormonal Shifts
Hormonal changes can accelerate or reveal an established pattern. In women, this may appear around menopause, in the postpartum period, or in polycystic ovary syndrome (PCOS). Exogenous hormones can also influence hair behavior, whether in bodybuilders using anabolic agents or in transgender patients on hormone therapy.
Recognizing Early Androgenetic Alopecia Patterns in Females

Androgenetic alopecia in women is often diagnosed later than in men because pattern loss in women does not always begin with an obvious hairline change. Common early signs include a widening central part, described as the Ludwig pattern, reduced ponytail thickness, and a more visible scalp under bright light. Some women show frontal accentuation, known as the Olsen pattern, while the frontal hairline itself remains preserved for a long time.
Early androgenetic alopecia female recognition matters because stabilization is easier before density loss becomes severe. When appropriate, assessment may include scalp photography, trichoscopy, and bloodwork covering iron status, thyroid function, vitamin D, and hormonal markers, alongside a medical history review.
Male Pattern Presentation and Progression
In men, androgenetic alopecia typically presents as temporal recession, frontal thinning, and vertex thinning, progressing along the general framework of the Norwood scale from minimal temple changes to more established crown and frontal loss.
For men considering future transplantation, early evaluation matters because donor planning is time-sensitive. A proper treatment plan should account for the currently thin area and also for likely future progression and donor reserve.
Androgenetic Alopecia Treatment Options
Medical Therapy
Medical therapy under physician supervision is often the first step. Topical or oral options may be considered depending on sex, age, pregnancy status, and medical history. Androgenetic alopecia treatment is primarily managed long term, and discontinuing therapy may allow progression to resume.
Regenerative Hair Regrowth Therapy
Regenerative hair support may be appropriate for select patients. For instance, at Vega, the approach taken uses bio-active signaling concepts including VEGF and PDGF Ultra Enhanced Media, alongside secretome-based cellular messengers that support follicular communication. It is not a comprehensive cure and is most useful while follicles remain biologically active.
Surgical Restoration
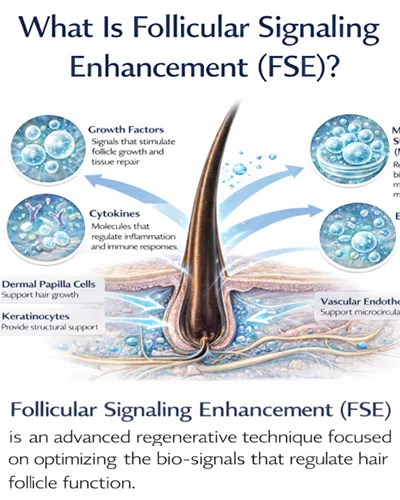
Hair transplantation may be considered when the pattern is stable enough and donor planning is suitable. Vega’s integrated model may combine transplantation with Follicular Signaling Enhancement, or FSE, to support graft response and scalp recovery during the post-procedure period.
Combination Planning
Single-modality treatment is often insufficient over the long term. Many patients benefit from a combined plan that includes medical stabilization, regenerative support, scalp health optimization, and transplantation only when the timing is right.
What to Expect From Long-Term Management
Pattern hair loss is managed rather than cured. Progression is typically gradual, and realistic outcomes may include reduced shedding, improved hair quality, partial regrowth in areas where follicles remain active, and surgical density restoration where appropriate.
For this reason, consistency across years is most important, and a good plan will describe what is likely reversible, what may only be stabilized, and what will require surgical restoration if the patient chooses that route.
Choosing a Hair Transplantation Clinic in Thailand
For international and GCC patients considering hair loss treatment in Thailand, important factors to evaluate include physician-led assessment, individualized natural hairline planning, donor-area protection, post-procedure regenerative support, and follow-up logistics suited to medical travelers.
Because of the nature of pattern hair loss and hair restoration, choosing a proper clinic that can handle the diagnosis, design, biology, and long-term planning is imperative for smooth outcomes.
When to Seek Consultation for Pattern Hair Loss
Consultation is recommended for patients with visible part widening, early temple recession, a family history of early-onset pattern loss, rapid thinning, or planned hormone therapy. Early evaluation expands the range of available treatment options and gives the treatment plan more time to work.
At Vega Dermatology & Wound Care Unit, our care for androgenetic alopecia begins with clinical evaluation to confirm the pattern and assess how far it has progressed. From there, we build a plan that may combine medical stabilization, physician-assessed regenerative hair regrowth therapy for suitable candidates, and surgical restoration where appropriate. Your progress is tracked over time and we adjust the plan as your stage of hair loss and long-term goals evolve.