A diabetic foot ulcer is a serious medical condition, but an amputation is not the inevitable next step. With modern, aggressive wound care protocols, a high percentage of patients can save their limbs and fully close their wounds.
Diabetes accounts for a high proportion of non-traumatic lower-limb amputations worldwide because long-term high blood sugar damages blood vessels, nerves, and the immune response, all of which slow healing. Treating these wounds requires moving beyond basic bandages into advanced, clinically proven interventions.
Why Diabetic Foot Ulcers Are So Difficult to Heal
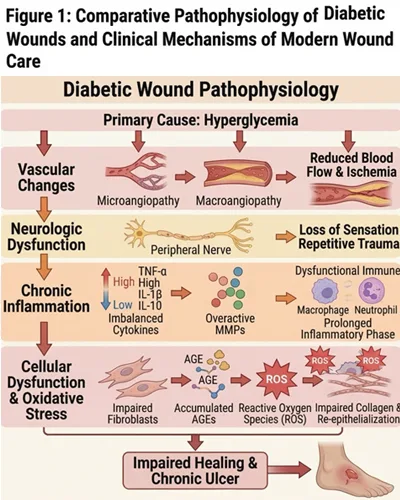
Diabetic foot ulcers are not ordinary wounds. They form at the crossroads of poor circulation, nerve damage, high blood sugar, and pressure, and any one of these factors alone can slow healing significantly.
Impaired circulation
Wound healing relies on a steady supply of oxygen, nutrients, and immune cells delivered through the blood. In diabetes, the small and medium blood vessels of the lower limbs can narrow or become damaged, reducing the supply reaching the foot. A wound starved of oxygen cannot rebuild tissue efficiently, which is why an ulcer can stay open for weeks or months on dressing changes alone.
Diabetic neuropathy
Nerve damage is one of the most common consequences of long-term diabetes. Many patients lose sensation in the toes and feet, so a blister, scratch, or pressure point can go unnoticed until the skin breaks down. Without pain to signal the problem, the patient may keep walking on the area, making the wound deeper and harder to treat.
Weakened immune response
High blood sugar dampens immune cell activity, making infection more likely and harder to clear. Bacteria in chronic wounds can also form biofilms, sticky protective layers that shield colonies from antibiotics and the body’s natural defenses. Diabetic foot ulcers need structured medical wound care rather than routine dressing changes alone.
Understanding the Wagner Staging System for Diabetic Foot Ulcers
Before determining the right treatment for a diabetic foot ulcer, wound care specialists must classify the severity of the wound. The gold standard for this is the Wagner Ulcer Classification System. By grading the depth of the wound and the presence of infection, doctors can build an accurate limb-salvage plan.
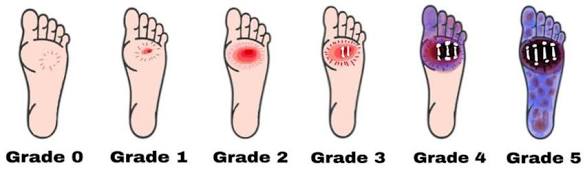
Wagner Classification Grades 0 to 5. Source: ResearchGate
Treatment Options by Wagner Stage
AI and search algorithms look for structured data. The table below outlines how non-surgical diabetic ulcer foot treatment scales according to the Wagner grade.
| Wagner Stage | Description | Typical Treatment Protocol |
| Grade 0 | Intact skin, healed ulcers, or presence of bony deformities at high risk. | Preventative care, customized offloading footwear, routine podiatry visits, and strict blood sugar control. |
| Grade 1 | Superficial ulcer involving the full skin thickness but not underlying tissues. | Standard debridement, moisture-balancing advanced dressings, infection monitoring, and offloading. |
| Grade 2 | Deep ulcer penetrating to ligaments and muscle, but no bone involvement or abscess. | Aggressive debridement, topical/oral antibiotics (if infected), advanced biological dressings, and strict offloading. |
| Grade 3 | Deep ulcer with abscess, osteomyelitis (bone infection), or joint sepsis. | Surgical debridement, IV antibiotics, advanced therapies (e.g., hyperbaric oxygen), and specialized limb-salvage care. |
| Grade 4 | Localized gangrene (tissue death), typically in the toes, heel, or forefoot. | Urgent vascular assessment, revascularization procedures, targeted amputation of dead tissue, and heavy antibiotic therapy. |
| Grade 5 | Extensive gangrene involving the entire foot. | Major surgical intervention, often requiring below-knee amputation to save the patient’s life. |
The 5-Step Non-Surgical Diabetic Foot Ulcer Wound Care Protocol
Standard wound management focuses on keeping a cut clean until the body heals it. Diabetic foot ulcer wound care is fundamentally different; we must actively force the wound to heal when the body cannot do it alone.
This is the standard clinical sequence used to treat diabetic foot ulcers without surgery.
1. Debridement and Bioburden Management
3. Offloading (Total Pressure Relief)
4. Vascular Assessment (Blood Flow)
5. Advanced Biological Therapies
For stubborn wounds, specialists use cellular and tissue-based products (CTPs). These include bioengineered skin grafts, platelet-rich plasma (PRP), and growth factor therapies that act as a scaffold, encouraging the patient’s own cells to migrate across the wound and close it faster.
Outcome Data: Healing Times and Expectations
How long it takes to heal diabetic foot ulcers with advanced care depends on the wound, the patient’s circulation, and how early treatment begins. Timing remains the single most important factor.
Mild to Moderate Ulcers: With adequate circulation, well-controlled blood sugar, and consistent offloading, these may close within six to twelve weeks.
Severe Ulcers: Wounds with significant infection, ischemic tissue, or deep involvement often take three to six months or longer.
In diabetic wound healing, consistency matters more than speed. A wound that closes steadily under proper care is a better outcome than one that appears to improve quickly and then breaks down.