Understanding Diabetic Foot Wounds and Ulcers
A diabetic foot wound is not an ordinary cut. It usually develops from changes that build up over time in the nerves, skin, and blood vessels of the foot, combined with pressure that the body can no longer sense or manage normally.
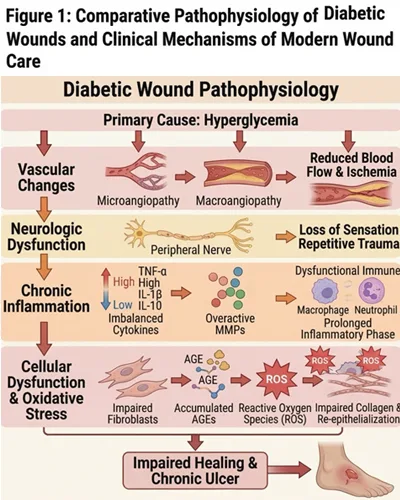
Three factors drive most cases: neuropathy, peripheral arterial disease, and repeated trauma. Diabetic neuropathy is present in a large majority of diabetic foot ulcers and works quietly by removing the body’s warning system. Without pain, pressure, or heat sensation, a small injury can worsen unnoticed. Neuropathy shows up in a few distinct ways. Motor neuropathy weakens the small muscles of the foot and can gradually reshape its structure. Sensory neuropathy reduces or eliminates the ability to feel pain and pressure. Autonomic dysfunction reduces sweating, leaving the skin dry, cracked, and more vulnerable to infection.
Peripheral arterial disease is also significantly more common in people with diabetes. Reduced circulation means the wound bed receives less oxygen and fewer nutrients, which slows healing considerably. Ulcers are generally classified as neuropathic, ischemic, or a combination of both, and this classification shapes the entire treatment plan, particularly for patients weighing options for diabetic foot ulcer treatment in Thailand as part of a broader medical tourism decision.
When to Seek Help for a Diabetic Foot Wound
Because diabetic foot wounds often cause little or no pain, the most important rule is simple: do not wait for pain before taking a foot wound seriously.
Seek medical attention if you notice:
- A sore, blister, or cut that shows no sign of healing
- Redness, swelling, warmth, or fluid discharge
- A callus with discoloration underneath it
- A wound that appears to be widening or deepening
- A foul odor, pus, spreading redness, or fever
A proper clinical evaluation covers the skin, circulation, nerve function, and the structure of the foot. One useful test is the ankle-brachial index, a simple, non-invasive measurement that compares blood pressure at the ankle and arm to check for arterial disease. The goal of early assessment is to identify a foot at risk before a minor issue becomes a severe one.
Core Principles of Diabetic Foot Wound Management
Effective diabetic foot wound management rests on a small number of established principles rather than any single treatment.
- Debridement: Removing dead tissue, debris, and callus that block healthy repair. This must always be performed clinically, whether surgically, enzymatically, biologically, or through controlled autolysis. It is never appropriate to attempt at home.
- Off-loading: Taking pressure off the wound, especially when it sits on the sole of the foot. Continued walking on an unprotected wound can damage the fragile new tissue forming underneath. Specialists commonly use total-contact casts, removable walkers, or custom therapeutic footwear to redistribute pressure.
- Infection control and a balanced wound environment: Ulcers tend to heal faster when infection is controlled and the wound is kept in a moisture-balanced environment with the right dressing, chosen based on depth, drainage, and infection risk.
- Addressing the wound’s underlying biology: Many chronic diabetic wounds have reduced local growth factor activity, which slows tissue repair.
- Advanced and adjunctive therapies: In selected, more complex cases, additional supportive treatments such as growth factor products, bioengineered skin substitutes, or negative-pressure wound therapy may be added on top of standard care.
At-Home Care for Diabetic Foot Wounds
At-home care does not replace professional treatment. It supports healing and helps prevent a small issue from becoming a larger one, which is central to how to heal a diabetic foot wound without setbacks between clinical visits.
- Check both feet daily, including the soles and between the toes, using a mirror or asking someone for help if needed. Do not rely on pain to flag a problem, since neuropathy can hide a worsening wound.
- Follow dressing instructions exactly. Keep the area clean and dry, wash your hands beforehand, and avoid unprescribed antiseptics or home remedies.
- Wear prescribed off-loading footwear consistently, even for short walks around the house, and check inside shoes for debris before putting them on.
- Never attempt to remove dead skin or calluses yourself. This significantly raises the risk of a deeper wound and infection.
- Support healing internally by managing blood sugar closely, avoiding barefoot walking, and avoiding smoking, which restricts circulation and slows healing.
- Watch for red flags. Contact your care team immediately if the wound grows larger, develops an odor, becomes warmer or more red, or if a fever develops.

Long-Term Management and Relapse Prevention
Diabetic foot wounds involve dermatology, wound care, neurology, vascular medicine, orthopedics, and endocrinology, often all at the same time. A complete care team may include a primary care physician, a wound care specialist and nurse, a podiatrist, a vascular surgeon, and nutrition support, each managing a different piece of the picture, from blood flow and structural alignment to blood sugar and dressing changes.
The risk of an ulcer returning remains high even after a wound has closed if pressure, footwear, circulation, and blood sugar are not managed over the long term. Prevention is not an afterthought once healing is complete. It is an ongoing part of care that includes protective footwear, pressure-point monitoring, and continued patient education to protect long-term mobility.
Book a Wound Care Assessment
A diabetic foot wound deserves early, specialized attention rather than a wait-and-see approach. A structured assessment can identify what is driving the wound and outline a plan that addresses both the active wound and the underlying vascular and neurological risk factors. Book a consultation with adiabetic wound care specialistat Vega Dermatology and Wound Care Unit for wound care or diabetic wound evaluation.
References:
- Diabetic Foot Ulcer. StatPearls. Retrieved July, 2026 fromhttps://www.ncbi.nlm.nih.gov/books/NBK537328/
- Diabetic Neuropathy. Retrieved July, 2026 fromhttps://www.niddk.nih.gov/health-information/diabetes/overview/preventing-problems/nerve-damage-diabetic-neuropathies