An oily scalp is uncomfortable on its own. Paired with more hair in the drain or on the pillow, it raises a reasonable question: is one causing the other?
Excess oil alone does not destroy follicles or produce the progressive, permanent loss associated with androgenetic alopecia. What oil does is shape the scalp environment in ways that can worsen existing hair loss and produce shedding.
Treating a scalp condition and treating hair loss are different problems, and identifying which one is in play comes first.
How An Oily Scalp Affects Hair Health
When sebum accumulates on the scalp surface, it holds onto dead skin cells, sweat, dust, and product residue. The resulting buildup creates a warm, low-oxygen environment at the follicle openings that can irritate the follicle and sustain low-grade inflammation over time.
The hair growth cycle then responds to that environment. Persistent irritation around the follicle can shorten the active growth phase and shift more follicles into the resting phase earlier than usual, producing diffuse thinning (overall thinning across the whole scalp rather than in specific areas like the hairline or crown).
What Causes An Oily Scalp
The scalp produces sebum continuously through sebaceous glands attached to each hair follicle. A normal amount of sebum waterproofs the skin, limits surface bacterial activity, and keeps the hair shaft supple.
When sebum production exceeds what the scalp needs, the excess accumulates between washes. For many patients, a persistently oily scalp is a biological baseline rather than a hygiene problem, and both genetics and external factors may contribute to the issue.
- Genetic factors: Baseline sebum production is partly inherited, which is why some families show consistently oilier scalps across generations.
- Hormonal influence: Androgens stimulate the sebaceous glands; higher androgen activity produces more oil.
- Hormonal fluctuations: Puberty, menstrual cycles, pregnancy, perimenopause, and menopause shift androgen activity and affect sebum output.
- Stress: Sustained stress raises cortisol, which indirectly influences sebaceous gland activity.
- Climate and humidity: Heat and humidity accelerate sebum production and spread, making oiliness more noticeable in warm environments.
- Product buildup: Heavy conditioning products, styling creams, and dry shampoos leave residue that mixes with sebum and is harder to clear.
- Cleansing habits: Infrequent washing allows accumulation; paradoxically, overwashing can also trigger a rebound increase in oil production.
Does Oily Hair Cause Hair Loss?
Oil does not damage follicles directly. What an oily scalp does is create the environment in which specific scalp disorders develop or worsen, and those disorders (not the sebum) may disrupt the hair growth cycle. Some scalp conditions that worsen with excess oiliness include:
- Seborrheic dermatitis: an inflammatory condition driven by the yeast Malassezia, which feeds on scalp oils; presents with itchy, flaky, and often red or greasy patches that can trigger diffuse shedding.
- Folliculitis: bacterial or fungal infection of the follicle opening, more common where oil and product residue accumulate.
- Dandruff: the mild end of the seborrheic dermatitis spectrum, producing visible flaking alongside oiliness.
Signs It May Be More Than A Greasy Scalp
An oily scalp on its own is a comfort issue. Paired with any of the following, it warrants a closer look, because what is visible on the surface may be connected to something progressing underneath.
Symptoms To Watch For
- Increased shedding: Noticeably more hair on the pillow, in the brush, or in the shower beyond the normal range of 50 to 100 hairs a day.
- Visible hair thinning: A wider part line, more scalp showing through the crown under direct light, or a reduced ponytail thickness.
- Persistent itching or irritation that does not resolve with standard shampoos.
- Persistent dandruff: Greasy, yellowish flakes that return quickly after washing may indicate seborrheic dermatitis rather than simple dryness.
- Visible scalp inflammation: Redness, scaling, or raised patches on the scalp surface.
When Clinical Review Is Recommended
Hair loss has many possible causes. Your scalp appearance alone is rarely enough to identify the primary driver. A clinical review with trichoscopy (a magnified examination of the scalp and follicles) can determine whether thinning follicles are present, if scalp inflammation is present, or if pattern hair loss is developing beneath the surface.
If you experience any of the following, it may be time to consider a clinical evaluation:
- Persistent hair loss for several months without improvement despite good scalp hygiene.
- Rapid or accelerating thinning over a short period.
- Patchy hair loss: Focal hair thinning rather than diffuse may point towards other causes.
- Family history of pattern hair loss, which increases the likelihood of progressive androgenetic alopecia.
Treatment Approaches For Oily Scalp And Hair Loss
Oily scalp and hair loss often coexist without sharing a cause. Effective care addresses both separately. Treating only the surface when pattern loss is also present will improve comfort but not density.
Improving Scalp Health
Scalp care is the foundation, particularly when inflammation or a scalp condition is contributing to shedding. The goal is to reduce the bacterial and fungal load on the surface, calm inflammation, and restore a balanced sebum environment without stripping the scalp entirely, which can trigger rebound oiliness.
- Appropriate cleansing frequency: Washing often enough to prevent buildup without overcleaning.
- Medicated shampoos: Formulations containing ketoconazole, zinc pyrithione, or selenium sulfide may be recommended under physician guidance for seborrheic dermatitis.
- Anti-inflammatory care: Addressing active scalp inflammation before applying any hair growth therapy, since inflammation affects how follicles respond.
Hair Restoration Therapies

Where hair loss has its own driver beyond the scalp condition, treatment needs to address that driver directly. The specific approach depends on what is causing the loss, its stage, and the patient’s overall health.
- Medical therapies: Physician-supervised options targeting the hormonal or inflammatory driver of hair loss.
- Scalp regeneration programs: Structured care focusing on the follicular environment and growth cycle support.
- Combination plans: Addressing scalp condition and hair loss simultaneously, since each influences the other’s treatment response.
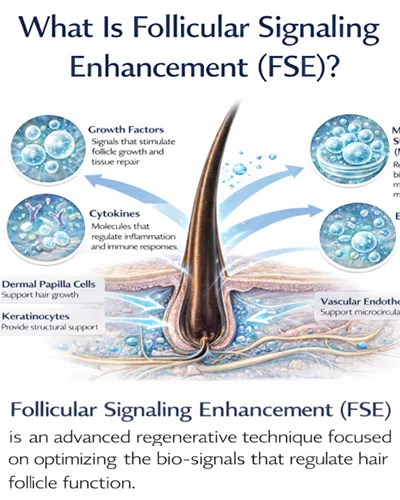
Advanced Approaches Focusing on Follicular Health
For suitable candidates where the follicle environment is the primary issue, regenerative protocols may help support the conditions follicles need to remain active. This is particularly relevant in cases where scalp inflammation has been identified as the main driver of hair loss.
Approach | Description | Suitable Candidate |
Bio-active signaling support | Secretome-based messengers and growth factor inputs such as VEGF and PDGF Ultra Enhanced Media, applied to support follicular activity and microcirculation. | Patients with low-grade scalp inflammation and a stressed follicular environment with follicles that are still active. |
A regenerative concept that aims to reactivate dormant follicles by upregulating molecular pathways such as Wnt/β-catenin and applying growth factors to support natural regrowth. Delivery is typically non-invasive, using microneedling or laser. | Patients with dormant or weakening follicles where the environment, not follicle destruction, is the primary issue. | |
Combination care | Regenerative support paired with medical or surgical therapy when both the scalp condition and the underlying hair loss driver need addressing. | Patients with both an active scalp condition and a separate hair loss driver such as pattern thinning. |
Final selection of any regenerative approach is made under individual physician assessment, taking into account scalp condition, the underlying cause of loss, and overall treatment goals.
When Hair Transplantation May Be Considered
Transplantation relocates healthy, DHT-resistant follicles from the donor zone to areas of established thinning. It addresses structural loss rather than the scalp environment, which is why it is rarely a first-line response to oily-scalp-related shedding. It becomes relevant only when pattern hair loss is confirmed, stable, and unlikely to recover without surgical input.
Diagnosis matters before any surgical decision. Book a consultation with our clinical team at Vega Dermatology & Wound Care Unit for scalp assessment or hair restoration planning. A physician-led review can identify any underlying causes that should resolve before surgical options become appropriate and determine whether structured hair restoration therapy may help your situation.
References:
- Seborrheic Dermatitis. Retrieved June 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK551707/
Hair Problems. Retrieved June 16, 2026, from https://medlineplus.gov/hairproblems.html - Hair Loss. Retrieved June 16, 2026, from https://medlineplus.gov/hairloss.html