What Is Regenerative Scar Therapy
Most scar treatments work on the surface. Regenerative scar therapy starts underneath it, in the tissue environment that decides how a scar forms and whether it ever fully settles.
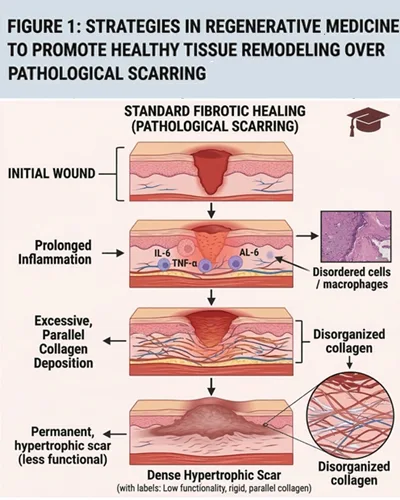
After surgery, skin moves through three overlapping healing phases: hemostasis and inflammation, proliferation, and remodeling. During this process, ordinary fibroblasts temporarily convert into myofibroblasts, contractile cells that help pull the wound closed. That step is healthy. The trouble starts when these cells fail to switch off. If they stay active too long, they keep depositing collagen the tissue no longer needs, producing raised, tight, or fibrotic scars. Keloid and hypertrophic scars sit at the extreme end of this pattern and share a common tissue signature: disorganized collagen, excess extracellular matrix, and an altered collagen I to collagen III ratio. For the patient, that translates to firm, itchy, uncomfortable scar tissue that often calls for a structuredscar tissue treatment plan rather than surface-level products alone.
Mesenchymal progenitor cells have drawn attention here because they do not work by replacing skin. Their influence comes through paracrine signaling, the molecules they release, which appear to calm inflammation, quiet overactive fibroblasts, and shift the local environment toward more orderly repair. For suitable candidates, the result may be a scar that softens, flattens, and moves more naturally. None of this is one-size-fits-all. Scar age, genetics, the tension in the surrounding skin, and any prior treatment all influence the outcome, which is why a proper clinical evaluation must come first.
Types of Cells Used in Surgical Scar Treatment
The phrase covers a wider range of options than most patients expect. The cell source, its preparation, and the delivery method all matter.
- Mesenchymal progenitor cells (MSCs): Multipotent cells capable of differentiating into several tissue types, but in scar work their value lies in the chemical signaling they release into the local environment.
- Adipose-derived progenitor cells (ADSCs): Collected from a patient’s own fat through a small liposuction step. Fat is a richer reservoir of regenerative cells than its reputation suggests, and ADSCs are easy to obtain from the patient without donor matching.
- Stromal vascular fraction (SVF): Keeps the whole biological mixture together rather than isolating one cell type. ADSCs, adipose precursors, endothelial cells, and immune-related cells act as a group, which may support blood vessel growth and coordinated repair.
- Bone marrow-derived progenitor cells (BMSCs): The longest history in wound-healing research. The effect appears to live in what they secrete rather than in the cells themselves.
- Secretome and extracellular vesicles: A shift in how the field thinks about these treatments. The molecular signals cells release, including exosomes and growth factors, may account for most of the therapeutic effect. What cells communicate matters more than whether they engraft long-term.

How Regenerative Therapy Reduces Surgical Scars Biologically
Surgical scars persist because the underlying biology has, in a sense, forgotten to stop. Understanding how to reduce surgical scars with stem cell signaling starts at this biological level, not just at the surface.
The TGF-β/Smad pathway sits at the center of most hypertrophic and keloid scarring. When it is dysregulated, it keeps myofibroblasts active long after the wound has closed, driving excess matrix deposition and the thickening that characterizes problematic scars. Signals from progenitor cells appear to interrupt this cycle. Specifically, mesenchymal cell secretions may shift the TGF-β1 to TGF-β3 balance, moving the tissue environment away from pro-fibrotic activity and toward the more orderly remodeling seen in normal skin repair.
Fibroblast overactivity is the other piece. These cells are essential during wound closure, but when they stay hyperactive, collagen keeps accumulating in tissue that does not need it. In research settings, secretions from bone marrow-derived cells have shown a measurable ability to calm this behavior and alter scar-related molecular signaling. Downstream, laboratory studies report lower alpha-smooth muscle actin, finer collagen architecture, and less chronic inflammation. This represents a change in scar biology rather than a change in appearance alone.
Clinical Techniques for Applying Cell Therapy to Scars
Technique selection depends on how the scar behaves, its depth, surface quality, tightness, and how it responded to any prior treatment. For patients considering medical treatment for keloids or hypertrophic scars, the following approaches are used in regenerative dermatology.
- Autologous fat grafting: Transfers the patient’s own fat, along with its naturally occurring regenerative cells, into and around scar tissue. It targets fibrosis, skin quality, and restricted flexibility at the same time.
- Cell-assisted lipotransfer (CAL): Enriches transferred fat with concentrated SVF or ADSCs. The added cellular density may improve outcomes in poorly vascularized scar tissue where standard fat grafting can struggle to survive.
- Nanofat preparations: A highly filtered fat preparation where regenerative components remain but intact fat cells largely do not. Best suited to superficial refinement of texture, tone, and fine-detail scar improvement rather than volume.
- Combination protocols: Layer regenerative support with laser resurfacing or microneedling to extend the remodeling effect beyond what either treatment achieves on its own.
Response varies by patient. Regenerative approaches are not a guaranteed cure, and outcomes depend on scar age, genetics, tissue tension, and treatment history, which is why proper evaluation comes before any protocol is selected.
Book a Specialist Scar Assessment
Raised, tight, or keloid-type scars respond best to a plan built around the specific tissue rather than a generic protocol. A specialist review can identify what is driving the scar’s behavior and which regenerative or combination approach fits your case. Book a consultation with our clinical team at Vega Dermatology & Wound Care Unit forscar care assessment and a personalized treatment plan.
References:
- Stem Cells Adaptively Respond to Environmental Cues Thereby Improving Granulation Tissue Formation and Wound Healing. Retrieved July, 2026 fromhttps://pmc.ncbi.nlm.nih.gov/articles/PMC7237390/
- Keloid and Hypertrophic Scars. Retrieved July, 2026 fromhttps://www.ncbi.nlm.nih.gov/books/NBK537058/