Burns are one of the most common skin injuries worldwide, and they range from minor irritations that fade in days to severe wounds that need months of structured medical care. The single most useful piece of information about any burn is its degree, because depth determines almost everything that follows: how it heals, what risks it carries, how much pain it causes, and what kind of treatment is appropriate.
Understanding the differences between first-, second-, and third-degree burns may help patients and caregivers respond appropriately when an injury happens and recognize when professional care is needed.
How Burn Stages are Classified
Burns are classified by depth, meaning how deeply the injury extends into the skin and the tissues beneath. The skin is a layered organ, and the burn degree corresponds directly to how many of those layers have been affected. The deeper the burn, the more biological repair the body must perform, and the higher the risk of infection, scarring, fluid loss, and longer-term complications.
Layers of the Skin Affected by Burns
Understanding the three primary tissue layers makes burn classification easier to follow.
- Epidermis: the outermost protective layer, responsible for barrier function and the visible appearance of skin. It contains no blood vessels of its own.
- Dermis: the middle layer that contains blood vessels, nerves, hair follicles, sweat glands, and most of the structures responsible for skin regeneration.
- Deeper tissues: subcutaneous fat, muscle, and in the most severe cases bone, which lie beneath the dermis and have very limited capacity to repair without surgical support.
A first-degree burn affects only the epidermis. A second-degree burn extends into the dermis. A third-degree burn passes through both, and deeper injuries may reach the tissues beneath. This depth-based system, sometimes called the classical or three-tier classification, remains the most widely used framework in clinical assessment.
First-Degree Burns
First-degree burns are the mildest category and the type most people will encounter in everyday life. The injury sits entirely in the outermost layer of skin, which means the underlying structures responsible for sensation, regeneration, and barrier repair are intact. Healing is usually straightforward, but recognizing a first-degree burn correctly matters because not every superficial-looking burn is as mild as it first appears.
Symptoms
- Redness, the most visible sign, caused by increased blood flow to the injured area.
- Mild swelling, usually subtle and resolving within a day or two.
- Tenderness or mild pain, generally well controlled with over-the-counter pain relievers.
- Dry skin without blisters; if blisters appear, the burn has reached the dermis and should be reassessed as second-degree.
Severity
- Affects only the epidermis, the outermost layer of skin.
- The mildest form of burn, generally managed at home with simple supportive care.
- Underlying structures responsible for sensation and regeneration remain intact.
- Heals within 3 to 6 days without scarring in most cases.
Common Examples
- Mild sunburn, the most familiar example, typically affecting larger areas of skin at shallow depths.
- Brief contact with a hot surface such as a pan handle, an iron, or a hot car seatbelt.
Treatment
- Cool (not cold) compresses applied to the area to reduce discomfort.
- Gentle moisturizers to support the skin barrier as it recovers.
- Over-the-counter pain relief if needed.
- Avoid further sun exposure or additional heat to the area during healing.
Second-Degree Burns
Second-degree burns are more serious. The injury has reached past the protective outer layer and into the dermis, where nerves, blood vessels, and the structures responsible for skin regeneration are located. This is why second-degree burns tend to be significantly more painful than first-degree burns and require more careful wound management. Healing time and scarring risk depend largely on how deep into the dermis the burn extends.
Symptoms
- Blisters, often the most distinctive sign, formed as fluid collects between the damaged layers of skin. The intact blister roof acts as a natural protective barrier.
- Significant pain, as nerve endings within the dermis are exposed to air and pressure.
- Appearance typically red, pink, or mottled, with visible moisture or weeping at the wound site.
- Swelling at and around the wound, sometimes extending well beyond the visibly burned area.
Severity
- Extends past the epidermis into part of the dermis, affecting some of the structures responsible for healing.
- More serious than first-degree, often requiring medical assessment for large burns, sensitive locations, or vulnerable patients.
- Infection risk increases once blisters break or if the wound is contaminated.
- Pigmentation changes may persist after healing, particularly in patients with darker skin tones.
- Superficial second-degree burns often heal without significant scarring; deeper second-degree burns commonly leave visible scars.
- Healing time ranges from about 2 weeks for superficial second-degree burns to several weeks for deeper ones.
Common Examples
- Scalds from hot liquids, including water, coffee, tea, or cooking liquids.
- Severe sunburn with blistering.
- Brief contact with flame.
- Hot grease splashes during cooking.
Treatment
- Gentle cleansing with water rather than harsh antiseptics.
- Do not deliberately break blisters; the intact roof protects against infection.
- Apply a clinician-recommended dressing and monitor for signs of infection (spreading redness, warmth, pus, or fever).
- Medical evaluation for burns that are large, on the face, hands, feet, joints, or genitals, or in vulnerable patients.
- Structured scar care may be appropriate for deeper second-degree burns once the wound has closed.
Third-Degree Burns (Full-Thickness Burn)
Third-degree burns represent the most severe category in routine clinical classification. The injury has passed completely through the epidermis and dermis, destroying not only the protective barrier of the skin but also the structures responsible for regeneration.
Because the body cannot rebuild this depth of tissue on its own, third-degree burns almost always require specialist medical care and frequently involve surgical reconstruction. Recognizing a third-degree burn quickly is critical, since delayed treatment increases the risk of infection, fluid loss, and lasting functional impairment.
Symptoms
- Appearance may be white, brown, black, or charred rather than the red associated with milder burns; this reflects the loss of normal tissue color.
- Texture often dry, stiff, or leathery to the touch, sometimes described as waxy.
- Reduced sensation at the deepest area because nerve endings in the dermis have been destroyed; surrounding less-severe areas often hurt more.
- A wound that feels relatively numb in the middle but painful at the edges is a symptom that the burn may be much deeper than it appears.
Severity
- Also called a full-thickness burn because the injury extends through the full thickness of the skin.
- Destroys both the epidermis and dermis, eliminating most of the structures the body uses to heal itself.
- In severe cases may extend into subcutaneous fat or deeper tissues, blurring the line with fourth-degree injuries.
- High risk of infection, fluid loss, and systemic effects, particularly when the burn covers a meaningful body surface area.
- The body cannot regenerate full-thickness skin on its own; specialist intervention is almost always required.
- Long-term considerations include scarring, contractures (skin tightening that limits movement), and rehabilitation that may take months or years.
Common Examples
- Prolonged exposure to flame.
- Electrical burns, where the visible injury often understates the underlying tissue damage.
- Deep chemical burns.
- Scalds from prolonged contact with very hot liquids.
Treatment
- Emergency medical care is required; home management is not appropriate.
- Skin grafting or reconstructive surgery is often necessary to close the wound.
- Structured multidisciplinary follow-up to address infection risk and functional impairment.
- Long-term rehabilitation for contractures, scar tightening, and functional recovery near joints.
- Ongoing scar care may continue for months or years after wound closure.
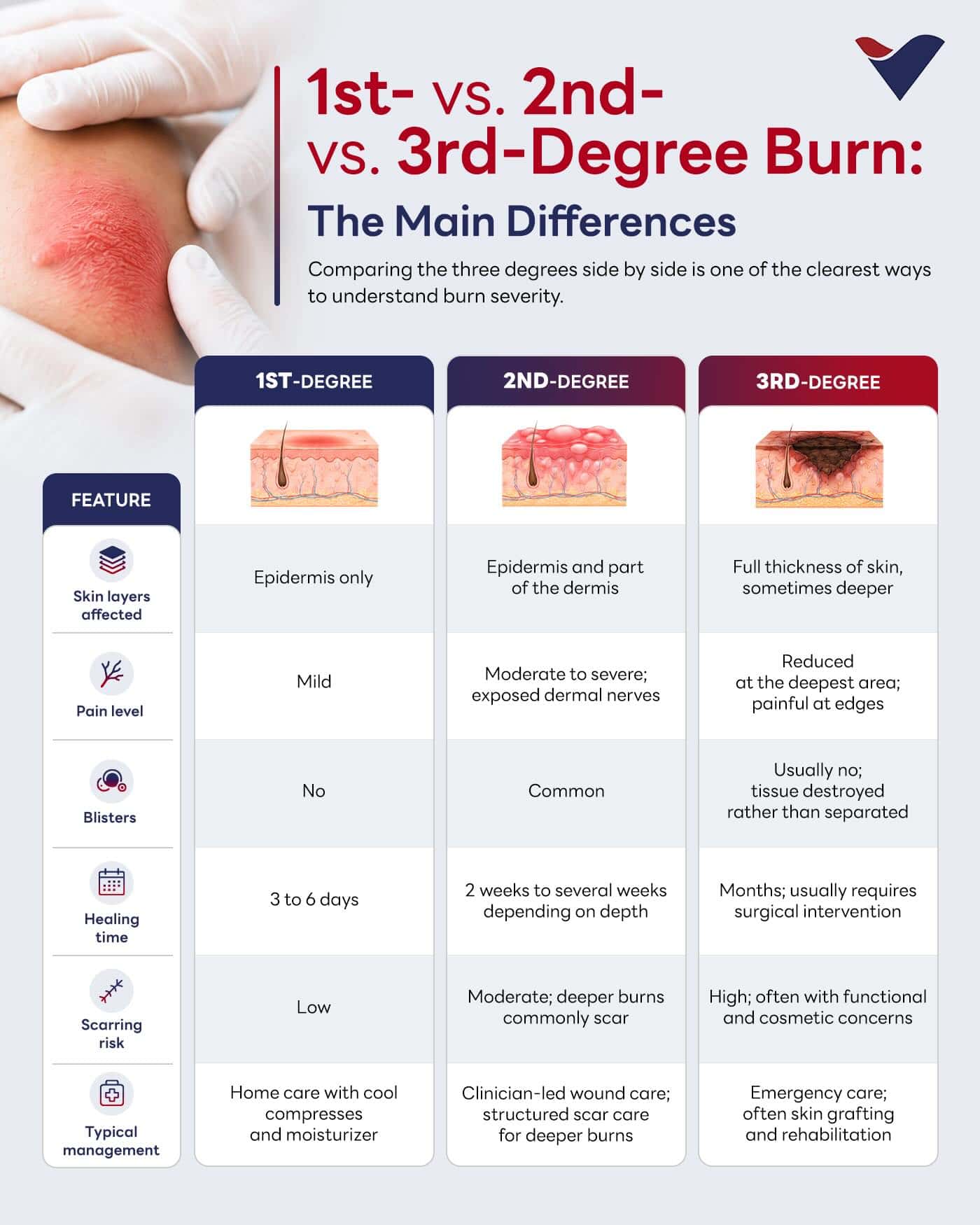
1st- vs. 2nd- vs. 3rd-Degree Burn: The Main Differences
Comparing the three degrees side by side is one of the clearest ways to understand burn severity.
Treatment Options For Burn Scars
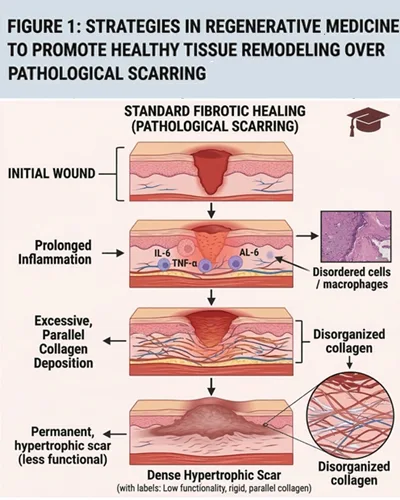
Burn scars can affect skin flexibility, restrict movement near joints, and produce ongoing itching or tightness. The depth of the original burn is the single biggest predictor of how the skin will recover, and several other factors, including wound care quality, infection, healing time, skin tone, and a personal or family history of keloid scarring, also influence the final result.
Begin your treatment for burn scars early and consistently for the best wound management. Several approaches may be combined depending on scar type, location, and stage of healing.
- Scar management therapies: Pressure therapy, silicone-based sheets or gels, regular moisturization, and ongoing sun protection to limit pigmentation changes.
- Wound care programs: Structured follow-up to monitor healing tissue and address concerns before they progress.
- Reconstructive and rehabilitation approaches: Appropriate for scars that restrict movement or affect function, particularly near joints.
- Supportive regenerative protocols: For suitable candidates, regenerative approaches under physician supervision may be considered as part of a staged scar care plan.
The earlier scar care begins, the more influence it can have on the final outcome. Even scars that have matured for months or years may still respond to physician-led intervention.

Improving Wound Management for Effective Scar Reduction
The first few days of wound management often shape how the skin heals over the months that follow, which is why timely clinical input matters even for burns that look manageable at first glance.
Importance Of Early Treatment
- Reduces complications: Prompt cleaning, dressing, and assessment limit secondary damage, infection, and tissue loss, all of which contribute to scar formation.
- Supports healing: Proper wound care shapes the trajectory of recovery, particularly in the first few days when the wound environment is most influential.
- May improve long-term outcomes, particularly for skin quality, function near joints, and visible scarring.
- Certain burns always warrant professional evaluation. Large burns, burns to the face, hands, feet, joints, or genitals, deep burns, electrical or chemical burns, and any burn in a child, older adult, or person with diabetes or circulatory conditions.
Waiting to see how a burn can heal on its own may cause unnecessary delays in supporting your skin integrity. When in doubt, having a clinical team review the wound is the safer route.
At Vega Dermatology & Wound Care Unit, scar reduction is approached as a pathway from the earliest point in healing rather than a single intervention after scars have formed.
- Physician-led wound assessment: Evaluation of burn depth, healing trajectory, and scar risk to guide a care plan suited to the individual injury.
- Scar care and tissue remodeling programs: Structured monitoring through scar maturation, with pressure therapy support, silicone-based options, and clinical follow-up as appropriate.
- Regenerative protocols for suitable candidates: Where appropriate, supportive approaches such as VEGF and PDGF Ultra Enhanced Media may be considered under physician supervision to support tissue conditions during healing.
- Continuity of care: The same clinical team manages assessment, treatment, and long-term follow-up, so scar care decisions are made with full visibility of how the original burn healed.
Early physician-led input is one of the most direct ways to support appropriate treatment for burn scars and protect long-term skin health. Book a consultation with our clinical team for wound care evaluation or scar care assessment now.
References:
- Burns Classification. Retrieved June 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK430741/
- Burns. Retrieved June 16, 2026, from https://medlineplus.gov/burns.html