Key Takeaways
- Scar tissue remodeling is the final wound-healing phase, lasting six to twenty-four months, during which scars can improve or worsen.
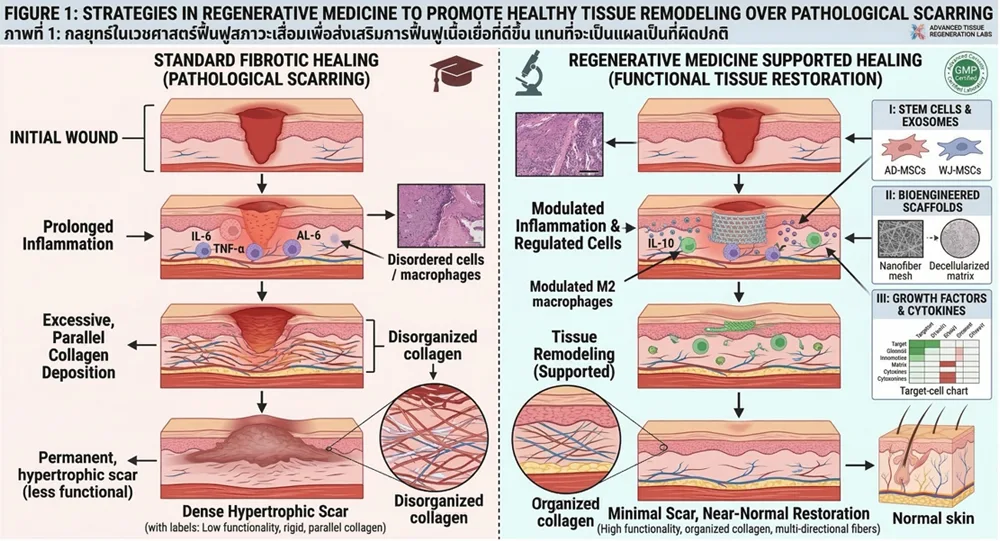
- Regenerative approaches aim to balance inflammation, fibroblasts, and collagen so healing moves closer to scar tissue regeneration rather than excess scarring.
- Treatment is matched to scar type, with different protocols for raised hypertrophic and keloid scars versus depressed atrophic scars.
- Earlier intervention within the remodeling window generally produces better outcomes than treating long-matured scars.
Every injury, surgery, or burn leaves behind some form of repair tissue. While scars protect and restore structure, abnormal collagen activity can leave skin raised, depressed, tight, or discolored. Advances in regenerative medicine are helping clinicians better understand how to guide this repair toward smoother, more functional outcomes.
What Is Scar Tissue Remodeling?
Scar tissue remodeling is the final stage of wound healing. After a wound closes, collagen fibers gradually shift from a disorganized patch to more aligned, stronger tissue. This phase typically begins around three to four weeks after injury and can continue for 6 – 24 months, depending on wound depth, location, age, and individual biology. Scars can improve or worsen during this window, which is why timely, targeted care can influence the final result.
Understanding Scar Formation
When the skin or underlying tissue is injured, the body initiates a complex and highly coordinated wound-healing process. This process typically occurs in several overlapping phases:
- Hemostasis – Immediate clot formation stops bleeding and creates a temporary protective barrier.
- Inflammation – Immune cells migrate to the wound site to remove debris, bacteria, and damaged tissue.
- Proliferation – Fibroblasts produce collagen and extracellular matrix (ECM) components to rebuild tissue.
- Remodeling – Collagen fibers reorganize and mature to strengthen the repaired area.
During the remodeling phase, which may last for months or even years, the initially disorganized collagen network gradually becomes more structured. However, when this process becomes imbalanced, abnormal scar formation can occur. Common types of scars include:
- Hypertrophic scars – Raised scars that remain within the boundary of the original wound
- Keloid scars – Overgrown scar tissue extending beyond the wound margins
- Atrophic scars – Depressed scars commonly associated with acne or tissue loss
- Contracture scars – Tight scars that may restrict movement, particularly after burns
The severity of scarring depends on several factors, including genetics, wound depth, inflammation levels, and mechanical stress on healing tissue.
The Biology of Tissue Remodeling
Tissue remodeling is the final and crucial stage of wound healing. During this stage, the extracellular matrix is reorganized to restore functional tissue architecture. Key biological mechanisms involved include:
- Collagen Reorganization Fibroblasts initially produce large amounts of type III collagen, which is rapidly deposited in the wound. Over time, this collagen is gradually replaced by type I collagen, a stronger structural protein that improves tensile strength.
- Matrix Metalloproteinases (MMPs) MMPs are enzymes that break down excess extracellular matrices. Their activity helps remove excess collagen and allows tissue to remodel into a more organized structure.
- Myofibroblast Activity Myofibroblasts are specialized cells that help close wounds by contracting the surrounding tissue. Once healing is complete, these cells normally undergo programmed cell death. If they persist, they may contribute to excessive scarring.
- Vascular Remodeling New blood vessels formed during early healing gradually regress or stabilize as tissue matures. Proper vascular remodeling ensures adequate oxygen and nutrient delivery during repair.
When these mechanisms remain balanced, scars may gradually soften, flatten, and become less noticeable over time.
Scar Tissue Regeneration vs. Scar Formation
Classic wound healing produces fibroproliferative repair that leaves a permanent scar. True scar tissue regeneration restores tissue architecture more completely, as seen in fetal skin and certain animal models. Adult human skin tends toward scar formation rather than regeneration. Current regenerative medicine cannot erase deep scars, but it may shift healing closer to regeneration by modulating inflammation, fibroblast activity, and matrix remodeling.
Types of Scars and How They Remodel
- Mature scars: flat, pale, and stable
- Hypertrophic scars: raised within the wound border from excess collagen
- Keloids: overgrown scars extending beyond the original wound
- Atrophic scars: depressed from collagen and volume loss, common in acne and stretch marks
- Contracture scars: tight tissue that can limit movement, often after burns
Scar tissue remodeling therapy and scar tissue treatment are selected based on scar type, with softening protocols for raised scars and volume- and texture-focused approaches for atrophic scars.
How Scar Tissue Remodeling Works at the Cellular Level
Fibroblasts and myofibroblasts produce collagen and help contract the wound. Over time, the matrix shifts from collagen III to stronger collagen I, while enzymes called matrix metalloproteinases break down excess tissue. Growth factors such as TGF-beta, PDGF, and VEGF coordinate this process. When signaling becomes unbalanced, scars may turn stiff, raised, or rigid. Regenerative approaches aim to rebalance these signals and encourage more orderly collagen alignment.
Factors That Influence Scar Quality
- Prolonged inflammation
- Poor oxygen supply or circulation
- Mechanical stress on healing tissue
- Wound infection
- Age and genetic predisposition
Emerging Regenerative Approaches in Scar Remodeling
Regenerative medicine focuses on supporting the body’s natural healing mechanisms. In recent years, researchers have investigated how biologically active therapies may influence tissue repair and scar formation.
These approaches aim to modulate inflammation, enhance cellular communication, and support healthy extracellular matrix remodeling.
Growth Factors and Paracrine Signaling
Cells involved in wound healing communicate through signaling molecules known as growth factors. These molecules regulate cell migration, proliferation, and tissue regeneration. Important growth factors in wound repair include:
- VEGF (vascular endothelial growth factor)
- PDGF (platelet-derived growth factor)
- TGF-β (transforming growth factor beta)
- FGF (fibroblast growth factor)
Balanced signaling from these molecules helps coordinate tissue repair while minimizing excessive scarring.
Cellular Messengers and Paracrine Signaling
Regenerative medicine research has shown increasing interest in how certain regenerative cells interact with the wound microenvironment. Rather than directly replacing damaged tissue, these cells primarily act through paracrine signaling, releasing bioactive factors that may:
- Modulate inflammatory responses
- Support angiogenesis (new blood vessel formation)
- Encourage healthy fibroblast regulation
- Promote balanced extracellular matrix remodeling
These mechanisms may help create conditions that favor more organized tissue repair.
Growth Factors and Paracrine Signaling
Another area of interest is the role of extracellular vesicles—tiny particles released by cells that contain proteins, RNA, and signaling molecules.
These vesicles may facilitate communication between cells during wound healing and may contribute to tissue remodeling processes.
While research continues to evolve, these biologically active components represent an exciting area of regenerative science.
Who Is a Candidate for Regenerative Remodeling Scar Tissue Care?
Suitable candidates may include patients with hypertrophic or keloid scars resistant to first-line care, or atrophic acne scars and stretch marks seeking texture improvement. Care is generally not recommended during active infection, uncontrolled systemic disease, or pregnancy depending on the modality. A physician-assessed consultation helps determine the right approach and set realistic expectations.
Scar Remodeling and Functional Recovery
Beyond cosmetic appearance, scar tissue can also affect functional outcomes. Excessive fibrosis may restrict tissue flexibility, impair mobility, or interfere with normal organ function.
For example:
- Burn scars may limit joint movement
- Surgical scars may affect tissue elasticity
- Fibrotic scars may alter nerve or muscle function
Strategies that support balanced tissue remodeling may therefore contribute not only to improved appearance but also to better functional recovery.
Timeline and Expectations for Scar Tissue Remodeling
Even with regenerative therapy, scar tissue remodeling is gradual. A general timeline includes:
- First 3 months: initial softening, reduced redness, and early texture changes may begin to appear
- 3 to 6 months: more noticeable improvements in pliability, height, and color
- 6 to 12 months: continued maturation, with scars becoming flatter, smoother, and less reactive
- 1 to 2 years: final remodeling phase, where long-term changes in tone, flexibility, and overall appearance stabilize
Realistic goals focus on:
- Improving pliability and flexibility
- Reducing scar height and thickness
- Softening scar borders
- Improving pigmentation and color match
- Easing symptoms such as itch, tightness, or pain
The aim is healthier, more functional tissue rather than fully erasing deep scars. Earlier treatment within the active remodeling window generally produces better outcomes than waiting years after a scar has matured.
Current Clinical Approaches to Scar Management
Several established clinical treatments aim to improve scar appearance and tissue remodeling:
- Silicone Therapy Silicone gels and sheets are widely used to help flatten and soften scars by improving hydration and reducing collagen overproduction.
- Laser Therapy Laser-based treatments may stimulate collagen remodeling and improve scar texture.
- Microneedling Microneedling creates controlled micro-injuries that trigger collagen remodeling and may improve atrophic scars.
- Corticosteroid Injections Steroid injections may reduce inflammation and collagen production in hypertrophic or keloid scars.
These treatments are often combined depending on the type and severity of the scar.
Future Directions in Scar Remodeling Research
The field of regenerative medicine continues to expand, and ongoing research aims to better understand how cellular therapies and biologically active factors influence tissue repair.
Areas of active investigation include:
- Regulation of fibroblast behavior during wound healing
- Controlled modulation of inflammatory pathways
- Enhancement of extracellular matrix organization
- Optimization of angiogenesis and vascular stability
Researchers are also exploring how personalized treatment strategies may help tailor scar management based on individual biological responses.
Conclusion
Scar formation is essential to healing, but the quality of the final scar depends largely on how tissue remodels in the months that follow. With evidence-aware care including silicone, laser, microneedling, and emerging regenerative approaches, patients can support healthier repair and improved long-term outcomes.



