Minor cuts and surgical incisions usually close within a few weeks. For some patients, however, the wound stalls instead of healing, where the skin around the edge stops moving inward, the wound bed looks unchanged week after week, and what should have been a short recovery turns into months of dressings and discomfort.
When a wound behaves this way, it stops being a simple injury and becomes a medical condition that needs structured evaluation. These are known as chronic wounds, and there are a few types.
When a Wound Is Considered Chronic
A wound is generally classified as a chronic wound when it fails to show meaningful, measurable signs of healing within 4 to 6 weeks of basic standard treatment. How long a wound is considered chronic can vary slightly by clinical setting, but 4 to 6 weeks remains the standard threshold across most wound care guidelines.
You do not always have to wait the full 6 weeks before seeking help. Early warning signs in the first 10 to 14 days, such as spreading redness, persistent odor, excessive fluid discharge, or worsening pain, are reasons to have the wound evaluated sooner. Early specialist input can reduce the risk of deeper tissue damage and complications, particularly in patients with diabetes, circulation problems, or limited mobility.
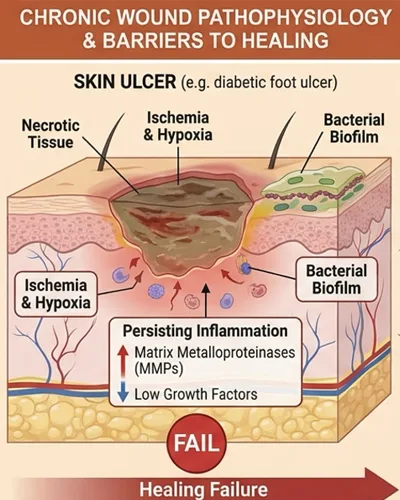
Why Chronic Wounds Get Stuck in Healing
Normal wound healing moves through four phases: hemostasis, inflammation, proliferation, and tissue remodeling. A chronic wound typically gets stuck in the inflammatory phase. Instead of shifting toward building new tissue, the wound stays in a prolonged inflammatory state. Consequently, cellular activity becomes dysfunctional, the signaling proteins do not switch off when they should, and the wound bed remains open and vulnerable.
This stalled state is rarely about the wound alone, as the healing process is often stalled by underlying issues, including poor circulation, uncontrolled blood sugar, sustained pressure on the area, persistent bacterial activity, or compromised nutrition. Addressing those root factors is usually as important as treating the wound itself, which is why a thorough clinical evaluation matters before any treatment plan is built.
The Main Chronic Wound Types Explained

Four chronic wound types account for the majority of cases seen in specialist wound care.
- Venous leg ulcers are the most common. They result from poor vein function in the lower legs, known as venous insufficiency. Blood pools in the lower extremities, raising pressure in the veins and damaging the skin from within. The result is shallow, weeping sores, usually on the inner lower leg around the ankle. These ulcers can recur even after they close if the underlying vein issue is not managed.
- Diabetic ulcers arise from a combination of nerve damage and reduced arterial circulation. Patients with neuropathy may lose sensation in the feet, so a small pressure spot or unnoticed injury can deepen into a stubborn ulcer before it is felt. Poor circulation slows the delivery of oxygen and nutrients needed for diabetic wound repair, and elevated blood sugar can affect the immune response that normally helps clear bacteria from the wound.
- Arterial ulcers are triggered by narrowed arteries, often from peripheral artery disease. Restricted blood flow means the feet and toes do not receive enough oxygen-rich blood. The resulting wounds are typically deep, painful, and slow to heal, and they are often found on the toes, heels, or outer ankle.
- Pressure injuries, sometimes called bedsores, develop when uninterrupted pressure on skin over bony areas, such as heels, ankles, or hips, cuts off blood flow. Tissue damage can occur quickly, particularly in individuals with limited mobility or reduced sensation, and the wound can extend deeper than the surface appearance suggests.
How Specialist Wound Care Can Support Healing
Chronic wounds rarely respond to off-the-shelf bandages because the underlying issue is usually upstream of the wound itself. At Vega Dermatology & Wound Care Unit, wound care begins with clinical evaluation, involving identifying the wound type, assessing circulation and any contributing conditions, and reviewing what has been tried so far.
From there, care is built around a structured pathway of wound bed preparation, infection control where needed, and advanced local care matched to the wound type. For suitable candidates, regenerative support such as VEGF and PDGF Ultra Enhanced Media may be considered under physician supervision as part of the wider plan. Tissue response is tracked objectively over time, with the approach adjusted as the wound progresses.
The clinical posture is conservative and protective, with the aim being to break a wound out of its stalled phase, protect surrounding skin, manage complications early, and reduce the likelihood of escalation. Even so, it’s important to note that treatment response varies depending on individual factors, including underlying health and the wound’s history.
When to Seek Specialist Wound Care
A wound that has been open for over a month is no longer a simple injury, instead being a chronic condition that benefits from professional management. Early specialist clinical action is the most reliable way to reduce the risk of deeper infection and other complications down the line.